
In the analysis of cardiovascular waveforms, certain derived variables maintain their value under transformations of the signal. These invariants are of particular interest because they offer robustness to variations in signal acquisition, calibration, and sampling. Invariant features are especially valuable in clinical research and automated signal processing, where measurement conditions often differ across devices, sites, and recording sessions.
Pressure waveforms obtained from catheter-based recordings, for example, may exhibit variability in amplitude scaling, baseline offset, or temporal resolution. Many commonly used variables are sensitive to such differences, which can lead to inconsistencies in comparative or longitudinal analyses. In contrast, an invariant retains its value under these transformations, provided that the relevant physiological landmarks are reliably identified.
A representative example is the pressure-based ejection fraction (PBEF), which is defined as one minus the ratio of end-systolic pressure (ESP) to isovolumic pressure (Pmax) [1]. The ESP corresponds to the pressure at the end of systole, while Pmax represents the peak pressure that would be reached if no ejection occurred. PBEF is invariant under amplitude scaling and under time-axis transformations such as temporal shifting or resampling.
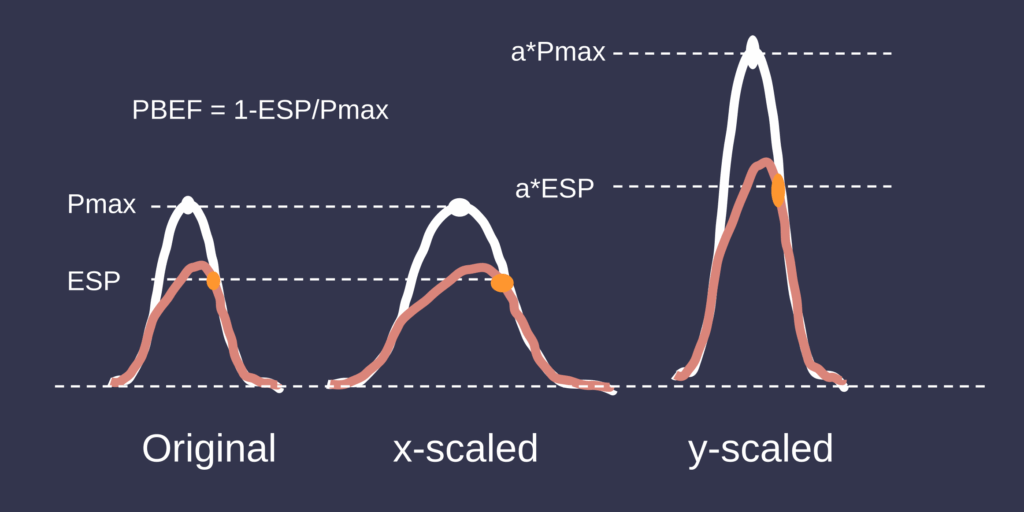
However, it is not invariant under vertical shifts of the pressure waveform. Adding a constant offset alters both pressures equally in absolute terms, but not in a way that preserves their ratio. As a result, the computed value of PBEF changes. This limits its applicability in datasets where the absolute baseline pressure is not reliably controlled.

In contrast, the augmentation index, commonly used in arterial pressure analysis [2], exhibits greater invariance. It is defined as the ratio of augmented pressure (AP) to pulse pressure (PP). The augmented pressure is the difference between the late systolic shoulder (or inflection point) and diastolic pressure. The pulse pressure is the difference between systolic and diastolic pressure. Since both the numerator and the denominator are pressure differences, the index remains unchanged under vertical shifts. It is also invariant under amplitude scaling, as both differences scale proportionally. This makes the augmentation index more robust to baseline drift and inter-device variability. However, its reliability depends on the accurate detection of waveform landmarks, particularly the timing of the reflected wave.
The formulation of invariant variables is not only a methodological consideration but also a means of isolating physiologically meaningful signal characteristics. In many cases, invariants correspond to fundamental mechanical or hemodynamic relationships. Their insensitivity to measurement artifacts reflects a physiological consistency that is desirable in both clinical and experimental contexts.
In the setting of automated analysis and data-driven modeling, invariants are particularly important. Features that generalize across heterogeneous datasets reduce the impact of measurement artifacts and improve reproducibility. Moreover, because invariants often encode conserved physiological relationships, they serve as interpretable and robust markers in both descriptive statistics and predictive models.
For these reasons, the identification and use of invariant waveform features remains a central objective in the development of reliable methods for cardiovascular signal analysis.
References
- Heerdt PM, Kheyfets V, Charania S, Elassal A, Singh I. A pressure-based single beat method for estimation of right ventricular ejection fraction: proof of concept. Eur Respir J. 2020 Mar 12;55(3):1901635. doi: 10.1183/13993003.01635-2019. PMID: 31771999; PMCID: PMC7885179.
- Murgo JP, Westerhof N, Giolma JP, Altobelli SA. Aortic input impedance in normal man: relationship to pressure wave forms. Circulation. 1980;62(1):105-116. doi:10.1161/01.cir.62.1.105